Diagnostic testing is recommended when the pretest probability of Lyme disease in a patient is moderate to high. This is the case when a patient has symptoms or signs that are characteristic of Lyme disease and when they have had possible exposure to infected blacklegged ticks in an area where Lyme disease occurs.
Before ordering diagnostic testing, it is important to consider:
For patients who present with classic erythema migrans rash who live in or have visited an area where Lyme disease is common, Lyme disease may be a clinical diagnosis. In the early stages of disease when erythema migrans is present, antibodies often have not yet developed, and serologic testing can be negative.
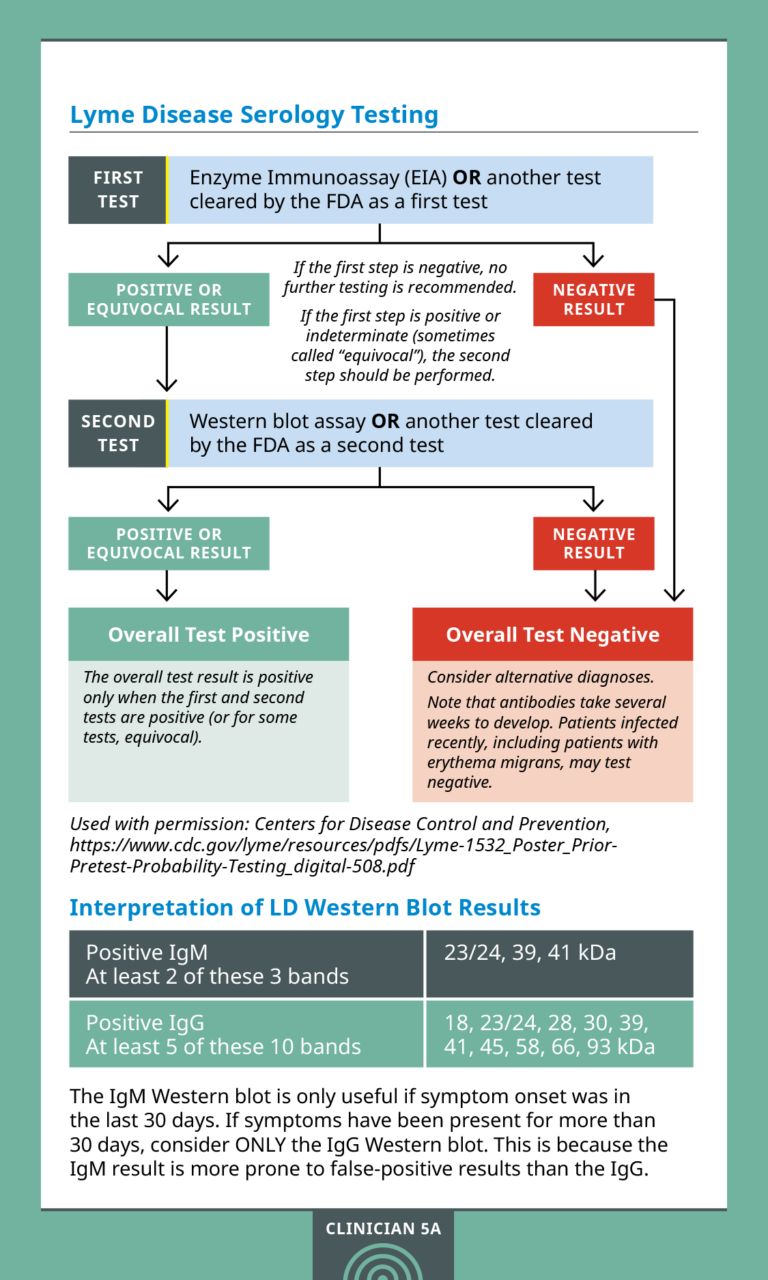
CDC currently recommends a two-step serum antibody (serology) testing protocol for Lyme Disease. Both testing steps are required and can be done using the same blood sample. If this first step is negative, no further testing is recommended. If the first step is positive or indeterminate (sometimes called “equivocal”), the second step should be performed. The overall result is positive only when the first test is positive (or equivocal) and the second test is positive (or for some tests equivocal).
Just like antibody responses to other illnesses, antibody response to the bacteria that causes Lyme disease takes time. In the days to weeks after a patient is bitten by a tick, they may test negative on serology tests in this early stage of the disease. A patient may present with erythema migrans and test negative, as the rash can develop within only three days of a tick bite. However, serology testing is highly accurate in later stages of infection, and paired convalescent serum testing to monitor for seroconversion may be helpful in some situations.
IgM and IgG responses can persist for years, so it can be difficult to distinguish between past infection with Lyme disease versus current infection. Multiple infections can occur, especially if the initial infection was treated promptly. You may need to rely primarily on clinical presentation rather than testing. False positives may also occur, particularly when pre-test probability is low. A patient infected with other diseases, including some tickborne diseases, or some viral, bacterial, or autoimmune diseases, may also receive a false-positive test result.
Lyme disease treatment varies in duration based on the presentation. Multidisciplinary guidelines for the prevention, diagnosis and treatment of Lyme disease are available for further information, including dosing information.
Doxycycline may be used for short courses (21 days or less) for children of any age. Studies have shown it is safe without causing tooth staining or weakening enamel. Patients who are 8 years of age or older may use doxycycline for any duration.
In general, antibiotic therapy after tick bites is not recommended to prevent Lyme disease. However, in certain circumstances, a single dose of doxycycline after a tick bite may lower a patient’s risk of Lyme disease. Prophylactic antibiotic therapy may be given to adults and children within 72 hours of a high-risk tick bite, but is not recommended for bites that are equivocal or low risk. Prophylaxis consists of a single dose of doxycycline 4.4 mg/kg (max dose 200 mg) for all ages.
If you cannot classify a tick bite as high risk, a “wait and watch” approach is recommended. Before recommending doxycycline prophylaxis, make sure that it is a safe medication for your patient.
Erythema migrans lesions in early Lyme disease may be diagnosed clinically. If the diagnosis is uncertain, consider serum antibody testing with repeat testing in 2-3 weeks if initial testing is negative.
Treatment for children of all ages may consist of one of the following regimens:
Doxycycline for 10 days
Amoxicillin for 14 days
Cefuroxime for 14 days
Second line antibiotics may also be available for patients in whom other antibiotic classes are contraindicated. Please refer to the 2020 Guidelines for the Prevention, Diagnosis and Treatment of Lyme Disease for specific treatment and dosing information.
Consider Lyme carditis in children who present with acute carditis of unknown cause with appropriate epidemiologic history. Serum antibody testing is preferred. PCR testing or culture of blood has poor sensitivity and is not generally recommended.
Treatment for children of all ages may consist of one of the following regimens:
Please refer to the 2020 Guidelines for the Prevention, Diagnosis and Treatment of Lyme Disease for specific treatment and dosing information.
Consider Lyme neuroborreliosis in children who present with acute cranial neuropathies or meningitis of unknown cause with appropriate epidemiologic history. Rarely in children, Lyme disease may also cause painful radiculoneuritis, mononeuropathy multiplex or spinal cord or brain inflammation.
Serum antibody testing is preferred. PCR testing or culture of blood or cerebral spinal fluid (CSF) has poor sensitivity and is not generally recommended. If CSF is obtained, it is recommended that simultaneous samples of CSF and serum are obtained for determination of the CSF:serum antibody index.
Treatment for children of all ages may consist of one of the following regimens:
Please refer to the 2020 Guidelines for the Prevention, Diagnosis and Treatment of Lyme Disease for specific treatment and dosing information.
Although a two- to four-week course of antibiotics cures most cases of Lyme disease, patients sometimes report symptoms of pain, fatigue, or difficulty thinking that last for more than six months after they finish treatment.
It is not known why some patients experience these symptoms. Studies funded by the National Institutes of Health have found that long-term outcomes are no better for patients who received additional prolonged antibiotic treatment than for patients who received placebo treatments.
Providers have an implied responsibility to use the newly acquired information to enhance patient outcomes and their own professional development. Any medications, diagnostic procedures or treatments discussed on this site should not be used by health care professionals without first evaluating their patients’ conditions, considering possible contraindications or risks, reviewing any applicable manufacturer’s product information and comparing any therapeutic approach with the recommendations of other authorities.